2011 has been a memorable year for MindHealthBiz. I hope I’ve helped steer some people in a positive direction with this bolg.
MindHealthBiz continues to evolve, focusing more on the core expertise, which incase you don’t know is Hands-on Electronic Health Record selection, implementation and vitalization. I’ve met some new friends this year, which inspires gratitude.
.jpg) I’ve also had some people from my past help me out in ways I could never foresee. A ton of “coincidences” have come my way, all positive.
I’ve also had some people from my past help me out in ways I could never foresee. A ton of “coincidences” have come my way, all positive.
I’ve had some personal trials this year, who hasn’t? I am convinced that every challenge has led me to a better spot. Perhaps it’s just the old addage “That which doesn not kill us makes us stronger”…I prefer to look at each one of these events and situatios in my life as gifts from the Universe.
Remember in 2012, Peace and Love is where it’s at! -T.
Read more →I know, I’ve belabored the “release of information” subject.
It’s good to know somebody else is thinking about this, and in a far-reaching way. SATVA, our industry’s software vendors’ association recently posted an interesting article on Behavioral Healthcare’s magazine that lays out the importance of a “consent to disclose” form (I’ve called it a Release Of Information form or ROI) in the Electronic Health Record (EHR). Without a single, signed form in common, disclosure of the consumer’s health information can’t be shared without breaking at least one of 32 federal and state laws that protect consumers’ confidentiality. The goal would be to make a common electronic form available in all EHRs and RHIOs in order to assure a consumer gets the best treatment from any healthcare facility he walks into and maintains health information confidentiality.
 Naturally, consumer records electronically shared among their professionals providing care can reduce duplicate tests, duplicate data input and other wasteful activities, and even prevent medication errors that could cause big trouble for consumers, simply because the professionals are acting as a team, not lone guns. None of these benefits can be realized without a solid, mutually accepted ROI or consumer consent agreement (same thing, I’ll stick with ROI for now)
Naturally, consumer records electronically shared among their professionals providing care can reduce duplicate tests, duplicate data input and other wasteful activities, and even prevent medication errors that could cause big trouble for consumers, simply because the professionals are acting as a team, not lone guns. None of these benefits can be realized without a solid, mutually accepted ROI or consumer consent agreement (same thing, I’ll stick with ROI for now)
SATVA even delivered a specification for the consent form, (amazing these guys agree on something given the competitive spirit in the software industry), stating a number of ways RHIOs are affected by the protective laws I mentioned above.
The ROI would deliver instant approval to share information, which means more timely treatment for the consumer and less pain, whether physical or emotional. Wouldn’t it be great if you moved from Oregon to New York and your new professional had access to your chart across the country when you came in for your appointment? That’s electronically possible now, except for the lack of an ROI.
So, why is this little stumbling block to all these benefits a problem, you ask? There must be a way to overcome the problems.
Right now, all it takes is a signed form to share the data between providers and that can be faxed. A major drawback of this system is that most providers have completely different forms to fill out, and filling out multiple forms them takes expensive professional time. Then there’s the clerical time and energy spent faxing different professionals for their specific ROI forms, getting them signed, and then faxing them back before the patient record is transferred. Then, depending on the professional’s legal limitations and technological status, the information sought (could be many pages) would need to be faxed, mailed or shipped. Now multiply all that effort and trouble by the number of physical and mental health professionals involved in the consumer’s care.
Oh, and next, multiply that by the number of consumers seeking care that day among all the professionals involved. The energy and expense both mount up.
I’ve commented quite a bit on Health Information Exchanges (HIEs) or Regional Health Information Organizations (RHIOs), and they’re key to this subject. RHIOs need to become intimately acquainted with those laws and rules I mentioned earlier…they have the same responsibilities to consumers as software vendors and professionals. This means the electronic ROI would need to be a common design among all the software vendors, professionals and their RHIOs, and also maintain the consumer’s stamp of approval and specific mention of the professionals involved, whether it’s an individual or an organization. That’s quite a job, too, but it can be done more simply and elegantly with electronic transfer of the health information data. The ROI also needs to cover why the consumer’s information is being shared; is the reason clinical, financial or something else? Since a RHIO can’t pass along information to anybody who’s a member without authorization, some sort of accountability needs to be built into the string of data sharing and availability to assure consumer confidentially.
Like I said, it’s a big job. The good news is that SATVA says they’ve already built it and have tentative approval of SAMHSA, and all the professionals and RHIOs need to do is buy it…but then again, maybe it’s free.
How likely is that?
Read more →The number of folks able to validate “best practices” with significant research data is startling…meaning it ain’t many.
There are a ton of “best practices”, or different “brands” of therapy in use across the nation with no single method of proving on a grand scale how well they work. Maybe if they were tracked in an interoperable Electronic Health Record (EHR), and shared among professionals, a handful of these methods of treatment would have the data needed to prove their worth. The fact is, we’re behind the curve in this.
 Recently H Wesley Clarke, director of SAMHSA’s Center for Substance Abuse Treatment shared his feelings on the condition of Health Information Technology in the field at the 2011 National Conference on Addiction Disorders, and he’s convinced that the EHR is under-deployed, to say the least.
Recently H Wesley Clarke, director of SAMHSA’s Center for Substance Abuse Treatment shared his feelings on the condition of Health Information Technology in the field at the 2011 National Conference on Addiction Disorders, and he’s convinced that the EHR is under-deployed, to say the least.
It’s all about data. Clarke understands that without analyzing the data that could be gathered using the EHR, professionals in addictions treatment are slow – as snails – to get the job done. In my experience, there are some professionals who believe documenting their treatment in the EHR slows them down and detracts from therapy. The question becomes, how do they know their brand of treatment, what they believe to be their “best practice” is the best way to help the consumer? Without documentation and a means to measure outcomes we’re relying on gut feeling, and when gut feelings are stood alongside outcomes measurement data, who knows whether they’ll be borne up unless we compare?
When a consumer paying for her own treatment (no insurance or Medicaid), she may want to know where her money’s going. She may respond better to the professional if there’s a study that can be quoted showing the effectiveness of the best practice she’s participating in. One thing I’ve learned after a number of years serving professionals with EHRs is that the more data you have, the more impressive the study. When I run across studies with absolutely huge data samples used to draw the conclusions, I’m inclined to believe the study’s true without even reading the study or book…call me trusting, but it’s trust based on data.
Assessments are the EHR‘s greatest tool to provide measurable outcomes…ask enough folks with substance abuse problems questions about suicide, and compare the results with people who lack the addiction disorder, and you start to see patterns. How do we know the measurement tool (the assessment) is worth its salt? Are we asking the consumer the right questions? Once we determine there is a danger of someone hurting themselves and we decide to treat it, how do we know that best practice used to treat that danger is the most effective treatment we can use?
Without data, we don’t know.
Without the EHR, our data can be insufficient. Without computer assistance, analyzing data just takes too long and is prone to mistakes in data compiling and analysis.
OK, so the EHR solves the local data problem in a professional practice, clinic or multi-location facility…When does it happen? There are a number of professionals who have used electronic documentation for a number of years, however the bulk of our field is in the dark…Email and Facebook on the work computer, and maybe Word documents about patients, which is a no-no when it comes to confidentially.
The EHR is the best tool going to help improve treatment. So, let’s get started, it will make H Wesley Clarke happy and is likely to save lives and help a bundle of consumers be happier, too.
That still leaves the question of how to get huge data samples an open issue. That requires interoperability and data sharing among professionals across the nation, and next time I’ll share some expert opinions (other than my own) on how to get that job done.
Read more →Executive Summary
New York State Medicaid Health Homes have been defined, including the offer of payment for providing the coordination of care among a network of providers required to be a Health Home. Providers are diligently completing applications (due November 1, 2011). Electronic communication to facilitate this coordination of care for Severely and Persistently Mentally Ill (SPMI) consumers is critical to deliver care in a reasonable amount of time. A prime goal for the Health Home is to reduce emergency room and hospital stays for these folks.
 This system of care is most efficiently managed with the help of interoperable software. An exploration of current thinking follows, discussing questions that have been raised in conjunction with efficient and effective planning to share data among Health Home network providers and the involvement of the Electronic Health Record (EHR) in this effort at the care provider level, and the involvement of the RHIO in securely sharing that patient data at the network level.
This system of care is most efficiently managed with the help of interoperable software. An exploration of current thinking follows, discussing questions that have been raised in conjunction with efficient and effective planning to share data among Health Home network providers and the involvement of the Electronic Health Record (EHR) in this effort at the care provider level, and the involvement of the RHIO in securely sharing that patient data at the network level.
Although the EHR is not required to be in place at the outset of the Health Home adventure, some system of communication throughout the Health Home network is required. Without an electronic solution with a modicum of automation, documentation and communication requirements for coordinating treatment for some consumers will be onerous. The requirement of a plan to have an EHR in place within 18 months for all care provider organizations involved with Health Homes seems like a lot of time to some. It’s not; there are too many project details involved to delay. A few software companies brag that they can have an EHR up and running in 90 days. That is likely true, MindHealthBiz actually uses similar rapid change cycle software implementation methods. Care providers on the other hand may falter in meeting aggressive targets simply because they don’t have professionals with requisite skills and bandwidth available to do the job in a short time frame. Implementing an enterprise EHR is a huge task in itself, and tackling electronic communications among care providers for a SPMI patient complicates the job…this is a completely new application for software that has only the foundation elements defined and not yet assembled.
Paying for EHR Software As usual, the first question that arises is “who’s going to pay for all this?”
HEAL grants have been suggested as a way to pay for EHRs at the provider organization level, as significant work will need to be performed to get software ready to securely and electronically share patient data among members of a Health Home network. A number of HEAL awards have been granted over the past few years with regard to sharing consumer information among care providers, as well as establishing regional centers for Health Information Technology (HIT) assistance. The results of these grants are available to providers if they choose to use them.
Currently, Meaningful Use incentives are the best bet in gaining revenue to offset the expense of software. A few software companies capable of deploying to a large HHS organization have gained certifications required to qualify to receive Meaningful Use incentive funds. Other software companies are in the process of earning the certification, or plan to apply soon. If a care provider agency plans to fund their EHR purchase with Meaningful Use incentives, there are a few things to pay attention to from the outset. • Currently an organization must apply for incentives through their eligible professionals (prescribers, usually doctors) (http://blog.samhsa.gov/2011/09/09/behavioral-health-organizations-begin-receiving-incentive-payments-for-health-it/) o For Behavioral Health, The Behavioral Health Information Technology Act of 2011 (S. 539) is active in the US Senate to establish more appropriate criteria (http://www.informationweek.com/news/healthcare/EMR/229301263) for our field, and expand the list of eligible professionals to include other licensed professionals o The current reimbursement is $63,750 per eligible professional…if you have ten doctors working, that’s a significant amount to be paid over five years. If you don’t you’ll need the aforementioned bill to pass in order to collect significant incentives for Psychologists and Licensed Mental Health Counselors • Thirty percent of the eligible professionals’ consumers served must be Medicaid funded • Core Measures (http://www.cms.gov/EHRIncentivePrograms/Downloads/EP-MU-TOC.pdf) are generally attested to by the EHR vendor, however the agency is responsible to use the tool and meet the requirements.
There are more details (like connectivity to SHIN-NY (Statewide Health Information Network for New York) to address and more measures to meet as the EHR is used. If we address the foundation elements above first, future requirements are designed to fall into place as long as the provider uses the EHR as intended according to the certification and follows the rules. Of course a gap analysis performed by a neutral party is appropriate due diligence for any organization planning to be included in a Health Home network.
Recently I performed a survey of major New York City providers, like New York City’s HHC, and discovered that the majority of hospitals and large human services provider organizations have no enterprise Behavioral Health EHR on line, and are either just now implementing, or more likely, engaged in a purchasing process for the software.
This last point is a stickler, and where providers of care can stumble a bit in doing what they need to do to continue collecting Meaningful Use incentives. Some agencies have created a full time position for this job, others contract with companies like MindHealthBiz to assure they collect the incentives without incurring penalties along the way. Participants in the Meaningful Use incentive program are required to provide on-going proof of performance like self-attestation that will need to be proven in order to avoid having to return incentives already paid.
Connectivity Who is your Regional Health Information Organization (RHIO)? Are they working with your software vendor? Answer these questions and you’ve started a project, so be prepared to have adequate human resources available with time, persistence and expertise to dig into the details. It is best for care providers to have a voice in development of any system regarding what data flows to what electronic destination, and exactly how it gets there. Software vendors have varying levels of knowledge and expertise in confidentiality requirements and exact workflow within care providing organizations. Your organization could be a model for development of the Health Home network plan for your vendor, with great say in product development. Act quickly.
The point of electronic connectivity is communication throughout a disparate, multi-provider treatment team, through the Health Home’s care coordinator / case manager. Technology exists for the software vendor and RHIO can enable this, and it’s necessary for them to cooperate with one another on exactly how the electronic communications will flow among treatment team members. Questions arise at the care-giving level: How do I know my consumer has seen another provider? Who owns the treatment plan, and how is it shared? What notes can/must I share? The list of elements that affect care at the provider level continues.
As shared earlier, it’s important to be involved from the outset with your EHR vendor and have some say in the development of how new functionality will work. Would you rather your professional staff guide the details of gathering and sharing consumer data, or a software company’s project manager and programming staff? This has been a pet peeve of mine in software manufacture; programmers seldom analyze several common workflows for the same task in different care provider settings. One very handy remedy to this problem has turned out to be the dual edged sword of designer tools that come included with software packages.
These tools can potentially help save a ton of development costs. On the other hand, if a care providing agency doesn’t know the vendor’s communications plan for the Health Home network or doesn’t want to wait for a solution they may develop their own technology with design tools. This can hurt the provider as the vendor follows its development roadmap at their intended, albeit usually slow, pace. Be aware of details like this and avoid mistakes that waste resources and money.
Oh, one more connectivity item in this short story….Managed Care for all NYS Medicaid is the next step for our world, so remember to garner some sort of electronic link to your EHR with your Managed Care Organization (MCO) or BHO. This avenue may provide valuable encounter data and speed authorization processes. The BHOs to move forward with have been (or are being) defined in your region, and that may or may not mean the provider agency is destined for big change for managed care.
A comprehensive Release of Information must be negotiated to meet requirements of the Health Home, 42 CFR, the other provider agencies in the network and other interested parties. My suggestion has been an electronic form provided through the RHIO that includes all network member agencies. I would like the ability to disclose the sorts of information that will be shared among agencies and give the option to the consumer to select which agencies he approves with checkboxes, or “all Health Home network agencies. Some plans laid for this adventure include only the latter, not the option for a consumer to pick and choose. That said, the consumer’s choice may boil down to costs being covered by Medicaid…or not. More will be revealed as the details are ironed out and the technology is fine tuned.
Of course, if you’d rather not rush into an enterprise EHR purchase, your RHIO may have a software solution they would be happy to provide for a monthly fee; you’ll still need to implement it, and that effort is still expensive in money and the provider agency’s human resources. This software would be an “Application Service Provider” (ASP) arrangement, and may be adequate for the interim period while agencies select their EHR. Just make sure the ASP software is certified for all ARRA purposes and you can live with the functionality limitations.
Functionality The right way to go about understanding shortcomings of software technology is to balance requirements with the reality of who enters what data where. A functionality grid fills in the blanks that are opened by a gap analysis and returns a “score” for each vendor involved. These grids are used commonly in Requests for Proposal, and can be limited to functionality needed to accomplish the goals of a Health Home. Some of the Health-Home-specific elements that should be considered include: • A robust referral module o Drop-down dictionary selections for all Health Home Network members for multiple screens involved in a consumer’s treatment o Other network care provider treatment and discharge information should be tracked as it may affect your care’s outcomes for the consumer (psychotropic medications, physical trauma, etc) • A Health Home Requirements Checklist to assure the Health Home Case Manager/ care coordinator has information required to make reasonable consumer care decisions; all providers involved need to share their findings and cooperate with one another, so the best solution would be interactive among care providers • The care coordinator will need live access to key data for utilization and quality reports from all Home Health Network providers • Treatment data transfer mechanisms compatible with a number of EHRs o Note: A number of formats are already in place for HIPAA electronic formats as well as tools like the Health Level-7 (HL7) to securely share demographic, clinical and transaction data…your vendor may or may not elect to use these standard formats, replacing them instead with their own proprietary mechanism; certification issues may ensue if that’s the case • A pool of funds is promised to Home Health networks for proving effective treatment: o What is the mechanism to measure improvement? o What is the base line for the measurement? o How is the data aggregated? o Are these Quality Control measures reflected in tools in each care provider agency’s EHR? • Account for the 3M Clinical Risk Groups within the EHR and entry of that data into the consumer record during intake and sharing the score with the multiple treatment team members • Immediate access to Diagnosis & Treatment data from other agencies & possible storage of some of that data in the patient’s local record. • Active tracking of available Health Home slots with Health Home Network interaction • Some required functionality may not be available from some vendors, however, if they intend to stay in business, there is a roadmap to comply with the requirements; Be aware, there may be additional costs to care providers • It is wise to track whatever a consumer does, counseling sessions, physical health treatment, even if they simply show up for activities, track their presence and reason for being in the facility • Document Imaging attaches electronic files like scanned treatment documents and fax files from other agencies to your EHR’s consumer record…All agencies in the Health Home network are required to have an EHR 18 months after the start date – until then, some will have little or no technology and rely on telephone calls and faxes until that time, so other members will need to account for recording conversations and attaching such electronic documents to the consumer record in their software; not all EHRs come with document imaging, sometimes they can be quite expensive to add into the mix
In Closing The Health Home goal of coordinating care for SPMI consumers is lofty, and has been proven effective in New York. For care provider agencies participating in the Health Home program, the EHR is a requirement, and a lot of work and inter-provider cooperation is involved in bringing it up to speed. There’s time to do this, however, with a task like this, a dedicated human resource needs to be involved in order to meet the 18 month requirement for completion and the likely wish to take advantage of Meaningful Use incentives to help pay for the EHR.
One critical aspect in creating a functional electronic network for the Health Home environment to communicate and coordinate consumer care is the willingness for the RHIO to work with a number of software vendors. Vendors tend to work with differing platforms. Even though they all may be ODBC compliant, they way they actually work can present challenges to communication. The jealously-guarded code and database behind the graphics we see can be as different as night and day among software programs. The RHIO’s willingness to work with all comers in this is only half the equation. Vendors will need to be willing to cooperate with the RHIO, other software vendors, and multiple care providers to define and possibly accept foreign methods of accomplishing the Health Home electronic communication goals. Be as certain of upcoming costs as possible, and understand an exact dollar amount is not likely to be available until the project is complete.
All focused functionality needs to be in place as soon as possible. Since this involves development on multiple platforms, a comprehensive plan is needed. It’s certain that at least some RHIOs and software companies are working on this, to their individual or partnership advantage. Are your RHIO and EHR vendor working together, or at least have an agreement to work together on the same plan?
Contact MindHealthBiz at 631-419-6879 or info@ehrsio.com to discuss details of your situation and how your agency can influence the process to implement an effective, efficient EHR solution. Leverage the earned wisdom of an IT professional required to advance your project to participate an electronically integrated Health Home network.
Read more →Treating drug addiction with drugs is nothing new.
Disulfiram, more commonly known as Antabuse has been around to help folks stop drinking since the 1920s…it makes the abuser sick if they drink. Methadone has been used for opioid treatment since the mid-1960s. These days, medications like Naltrexone are used to treat both opioid and alcohol dependence. The word is these drugs take the edge off the craving, which can be a key motivator to relapse.
 A difficulty in the past has been in actually tracking the prescriptions and medical treatment associated with treatment. In the 1990’s I worked with Gus Johnson, who invented a low-cost, comprehensive software system that tracked methadone and other medication prescriptions and administration with a link to specific consumer records; everything from writing the doctor’s order to dispensing was handled by the software, automatically saving all treatment records. Since then, a few companies like Metha-Soft and SMART have been moderately successful, resulting in a number of specialty software programs that work just fine for these purposes. These software programs are very focused to the clinic environment, and may not seek certification required to participate in ARRA funding to pay for software upgrades.
A difficulty in the past has been in actually tracking the prescriptions and medical treatment associated with treatment. In the 1990’s I worked with Gus Johnson, who invented a low-cost, comprehensive software system that tracked methadone and other medication prescriptions and administration with a link to specific consumer records; everything from writing the doctor’s order to dispensing was handled by the software, automatically saving all treatment records. Since then, a few companies like Metha-Soft and SMART have been moderately successful, resulting in a number of specialty software programs that work just fine for these purposes. These software programs are very focused to the clinic environment, and may not seek certification required to participate in ARRA funding to pay for software upgrades.
Where are the affordable comprehensive Electronic Health Records (EHRs) for small agencies? It’s getting tough for a clinic to focus only on opioid treatment or just alcoholism, since clinics are becoming increasingly involved in associated behavioral health and physical health issues. Larger software companies with an enterprise approach to electronic documentation and workflow management are certainly available, some with associated addiction treatment functionality, while others may not see an advantage to developing all the special features required in addiction treatment. Playing in that ballpark usually involves developing a bundle of said development by the software company, plus screen design and reporting tools that come with the system. If that advantage isn’t available, professional organizations generally get stuck with a never-ending series of development fees. In either event, some skilled human being needs to get paid for the development (good news for MindHealthBiz, since that work is part of the business).
Enter the almighty dollar.
Today, addiction treatment for a high number of consumers is funded by Medicaid, and not as many, but some, by Medicare. As incentive to use the EHR, beginning in 2015, Medicare payments will start to decrease for treatment agencies not using a certified EHR in a meaningful way. Medicaid doesn’t seem to have the same across the board penalty, but Medicaid programs are in financial jeopardy. Medicaid payments may also be affected for consumers who also have Medicare coverage. The skeptic in me suspects the decreases pioneered by Medicare may follow in future Medicaid adjustments.
Decreasing funding makes it tougher still to pay for the software update required to deliver an effective EHR and billing engine to professionals with all the right functionality for outcomes tracking, billing, etc. All this functionality is great stuff that benefits the consumer, however it all costs money in one way or another.
The upshot of this discussion is that smaller agencies need certified Electronic Health Records in order to improve their technology and track prescribing of these new medications. Enterprise (software that handles all an agency’s data and reporting needs) EHR software vendors are in a rush to get certified, so they can quite simply stay in business. In order to do that, the software is required to have an electronic prescribing capability, along with the ability to share patient data with Regional Health Information Organizations, (RHIOs), Health Home networks (http://www.health.state.ny.us/health_care/medicaid/program/medicaid_health_homes/)and organizations providing or tracking care to consumers from multiple care providers. The kinks are currently being worked out regarding consumer confidentiality, and that will be successful, I have no doubt. Smaller, specialty software vendors like the companies mentioned above have quite a challenge ahead of them.
Read more →I don’t believe it.
I’ve reviewed telemedicine a few times and new information about the subject grabs me. I recently heard a professional question the effectiveness of telemedicine, and since I hadn’t looked into studies about this, it seemed prudent to discover whether new effectiveness studies had overruled my previous positive opinion.
 I’ve been a supporter of telemedicine for mental health and substance abuse recovery and treatment, and if anything, the presence of electronic solutions are being used more and more. Electronic resources have been around a while, including apps for iPhones and BlackBerry smartphones with links to addiction recovery materials whenever the consumer feels like they need a quick recovery tune-up. The ability to perform and possibly record sessions for consumers in remote areas using computers’ cameras and microphones to bring people into a virtual session sounded nothing but good and research backed that opinion up, so it hasn’t occurred to me to question its effectiveness till now.
I’ve been a supporter of telemedicine for mental health and substance abuse recovery and treatment, and if anything, the presence of electronic solutions are being used more and more. Electronic resources have been around a while, including apps for iPhones and BlackBerry smartphones with links to addiction recovery materials whenever the consumer feels like they need a quick recovery tune-up. The ability to perform and possibly record sessions for consumers in remote areas using computers’ cameras and microphones to bring people into a virtual session sounded nothing but good and research backed that opinion up, so it hasn’t occurred to me to question its effectiveness till now.
A ton of supportive resources are on the internet and it turns out that electronic solutions are varied and well suited for a number of purposes.
I’ve covered therapy sessions via secure internet connections, and discovered that the availability of video in the session delivers the great benefit for the professional to better gauge the consumer’s body language…it can be difficult to pick up guarding postures and crossed legs and arms on the telephone. If you’re interested in telemedicine for mental health, you can see Demos and connect with one of the experts Secure Health. There are a number of companies providing secure telemedicine services, which is important, giving the nature of our industry, just search the internet to see other companies. There are just too many to mention here.
Last year CNN published a story on this subject citing an increase of success in depression treatment from 24 percent to 38 percent when on-line sessions were added to the treatment mix.
Telemedicine for mental health includes more than on-line sessions. In addition to the apps mentioned above, how about an Email or text on the smart phone to professionals for spot checks when a consumer feels off base. A few seconds spent with this technology could help bring a person into focus on recovery instead of relapse (there are security and confidentiality issues with this, so connect with a professional prior to moving ahead with this). Like a number of people, I think and process better either writing or by using pictures in a computer slide show. For folks like us, the solution of electronic communication with professionals can help us consider our thoughts and actions, and reflect on advice shared with us in past and in current communications.
The published account questioning effectiveness of telemedicine for mental health turned out to be rumor, anecdotal, without much support. I certainly support questioning effectiveness of any treatment in our industry, including the use of technological tools. This question, however, like Mark Twain’s famous quote, is the rumor of a death that’s greatly exaggerated.
Sheesh. I can get a kick out of sensationalism and exaggeration (I do that for fun sometimes), like most Americans (just watch the news to verify this), and the levels of that sort of thing has given me a healthy skepticism. I don’t believe everything I read. I’m glad to see there’s a growing interest in and value to telemedicine for behavioral health
Read more →It was doomed from the start.
Long ago, but not so far away I researched Google Health . When I checked out the service, it seemed like a great place for my primary care provider and specialists in cardiology or mental health to electronically transfer the records. Demand drives services like this, and in the end, the demand just wasn’t there for Google’s service. Partly because the demand wasn’t there, partially because it takes programming effort for a software company to meet other software companies’ requirements to securely transfer data, the service didn’t make it.
 It takes a special sort of programmer (aka expensive programmer) to develop secure data transfer technology, and security is the key concern when transferring health care data. Software companies are becoming less and less interested in doing this sort of work in the hopes it will pay off, simply because they’ve developed too many programs that didn’t. The Health Level 7 (HL7) format for transferring data is a good one, and really the standard that’s in use today. Most companies have developed this technology. It’s a matter of mapping data from an element in one program to the right spot in another program, say, like from your mental health or addictions professional’s office to Google. The problem is that every time it’s done, there are so many elements to account for in so many different ways, programmers commonly are re-inventing the wheel to get the right data from point A to point B in a secure fashion. It seems every software company approaches this common solution differently. That takes development, and as I shared, development is expensive. Professionals don’t want to spend the money, so data transfer programs, even those based on HL7, don’t get developed.
It takes a special sort of programmer (aka expensive programmer) to develop secure data transfer technology, and security is the key concern when transferring health care data. Software companies are becoming less and less interested in doing this sort of work in the hopes it will pay off, simply because they’ve developed too many programs that didn’t. The Health Level 7 (HL7) format for transferring data is a good one, and really the standard that’s in use today. Most companies have developed this technology. It’s a matter of mapping data from an element in one program to the right spot in another program, say, like from your mental health or addictions professional’s office to Google. The problem is that every time it’s done, there are so many elements to account for in so many different ways, programmers commonly are re-inventing the wheel to get the right data from point A to point B in a secure fashion. It seems every software company approaches this common solution differently. That takes development, and as I shared, development is expensive. Professionals don’t want to spend the money, so data transfer programs, even those based on HL7, don’t get developed.
When I originally looked into Google’s service, I didn’t think the electronic sharing of data was even available, so I saw no value. If it was available, it still requires cooperation from other software companies, and getting competitors to cooperate is a tough and expensive task. If electronic data transfer isn’t available for a scheme like storing my health data in a third party location, then I would need to either do some scanning or manual data entry, and I wasn’t (and still am not) up to either. Besides, patient portals are on the horizon. Patient portals are one answer to a new government mandate that healthcare data, like mental health treatment plans, be available to the consumer. It’s much better than printing a book for every patient who wants a copy of their health record.
I use the Veteran’s Administration as my primary healthcare provider, as well as a few clinics, however my cardiologist is special…I go to an outside professional for that. In order to assure the VA’s system is up to date, I get scanned records from the cardiologist, and that’s almost too much work for me. Sometimes the scans just don’t make it to the VA. Shame on me.
By the way, my heart’s healthy and strong like steel, with apparently no danger of heart attack eminent in case you’re interested.
In our world, everybody’s concerned with confidentiality….I wouldn’t want notes from a private therapy session with a professional released to anybody, and that’s a common feeling. This prevailing attitude makes it awfully tough for third party services like Google Health to make it.
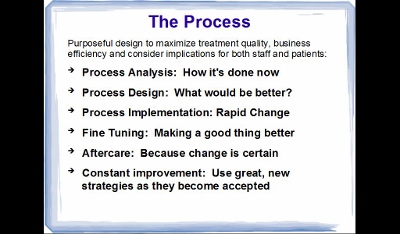
Read more →“Implementing an EHR may very well be the single largest project you will ever be a part of in your career”.
Believe it. I would add that if your organization’s EHR implementation wasn’t effective, the solution is to take a different look at how it’s done and plan to optimize what you have…read on.
 The statement above came from an announcement of a NIATx presentation I received recently. In the past, the biggest problem standing in the way of effectively and completely implementing an Electronic Health Record (EHR) for Mental Health and Substance Abuse Treatment was a reluctance to spend valuable professionals’ time and energy that’s required to be successful and make the software do what you want it to do. This could apply to any system, really, from a single provider to a large organization with hundreds of users.
The statement above came from an announcement of a NIATx presentation I received recently. In the past, the biggest problem standing in the way of effectively and completely implementing an Electronic Health Record (EHR) for Mental Health and Substance Abuse Treatment was a reluctance to spend valuable professionals’ time and energy that’s required to be successful and make the software do what you want it to do. This could apply to any system, really, from a single provider to a large organization with hundreds of users.
There are a number of approaches to getting the same thing done that all revolve around the same thing: Make the software do what the organization needs. I find that if we look at a few elements at a time, and note people who might be appropriate to head up that aspect of the implementation, we’re more likely to have a successful effort than if we try to blast everything out at once, disrupting the work and lives of every professional and treatment of every consumer.
Here are a few ideas to spur some thought, starting with what I think is most important, and then a couple different aspects of the broader view from experts in getting jobs done.
McLeod’s Method:
A call this “my” method, simply because it’s part of the system I use.
 Over the years I’ve picked up a bundle of experience and wisdom from so many sources it would be silly for me to go back and re-construct history….so I call it “mine”. There are many other factors to consider, so I also pay attention to the points attended to by industry leaders in their views below…and more. First, address these bullet points and look into elements like “Rapid-Cycle Change”.
Over the years I’ve picked up a bundle of experience and wisdom from so many sources it would be silly for me to go back and re-construct history….so I call it “mine”. There are many other factors to consider, so I also pay attention to the points attended to by industry leaders in their views below…and more. First, address these bullet points and look into elements like “Rapid-Cycle Change”.
Malcomb Baldridge The National Institute of Standards and Technology (NIST) Baldridge Award is a government award for excellence that includes criteria for healthcare for both profit and not for profit organizations. The reason to participate is, according to David Spong, former Boeing executive and winner of the award, is that it improves performance. For professionals, that means not only “production” (seeing more consumers), but improving consumer care for better outcomes. The Baldridge Criteria focus on several elements of importance and help health care organizations achieve and sustain the highest national levels of • Patient safety and loyalty • Health care outcomes • Professional staff satisfaction and engagement • Revenue and market share • Community services
Using the principles and processes of the Baldridge Criteria can’t help but improve an EHR implementation.
NIATx Pointers In a presentation from 2010, NIATx highlighted a number of important points you can use as a guideline in selecting and implementing the EHR. • Why purchase an EHR at all? It may be better for professionals and consumers for the organization to optimize what’s already in place • Is your organization ready? While you’re at it, consider transparency to the consumers and helping them get ready • How do I select a vendor and product? There are tons of approaches: take care, you may want to hire a professional • What about Project Management? Start planning the project prior to purchase so you know what you’re getting into • How does the Implementation affect the entire organization • How do I want to go about training staff and changing business processes to work better for consumers? • What’s the best “Go-Live” strategy? As I’ve said, I’m a big fan of implementing one piece at a time for a bunch of reasons we can talk about later • What are the benefits and problems associated with the EHR implementation?
I don’t mean to sound like a commercial for NIATx, it’s just a good resource. For interested professionals, a NIATx EHR Implementation web presentation is scheduled this week. Given opportunity I plan to listen in, and since I’m a little tardy in posting this, check in with the NIATx website or give them a call to see a copy of the presentation.
Then again, if your organization doesn’t have the people power to manage this sort of effort, and the writing is on the wall that it must be done soon, you may want to consult a professional like yours truly for some help.
Read more →On June 21st, I published my comments on Facebook for business…I just didn’t know it had become so important to augment a business site with a Facebook presence. Now I know. Interestingly, the visits to my website jumped by fifty percent for the month. I believe that was simply because Facebook is so doggone popular and my blog came up in the search engines more.

I recently attended the NIATx conference in Boston, and H Westley Clark, Director of CSAT (http://www.samhsa.gov/about/csat.aspx) was a featured speaker. He mentioned in his address that one of the difficulties in delivering treatment documentation to consumers is that it may end up on Facebook. This brings up aspects of confidentiality that are important not only to the consumer, but also to the professional and even the organization they work for.
The Electronic Health Record (EHR) is becoming more and more expansive these days. In addition to the assessments, treatment plans and progress notes, you might see brain scans or even recordings of telemedicine sessions. I asked Jim Mountain, a vendor of telemedicine software, about recording sessions. He advised that it can certainly be done, however, would a professional want to do to that when there’s a danger it could end up on YouTube? All the systems I’ve seen (and I’ve seen a ton) have proven secure, and hackers are not likely to effectively plumb for health information, however, all health records are available to consumers, who might make a decision to share portions of the record on social media. If you’re a professional, consider how you’d feel if your notes were shared that way, or your sessions broadcast.
I believe the consumer’s health record is their property as much as the professionals and the organization they work for. It needs to be guarded, and is. A friend of mine manages a business that protects the consumer identity of methadone treatment recipients from the state…42 CFR prohibits even the state from knowing the identity of consumers they are paying for with Medicaid. The point of this is protection. It’s pretty good these days as long as records aren’t accessed on a lost laptop computer or published on Facebook or YouTube. I doubt it’s likely to happen, but it could. Perhaps an agreement between the consumer and the professional to keep the record that’s provided to the consumer confidential is in order.
This is a huge issue. A couple years ago, Duke FUQUA School of Business published their take on just how huge it is. And they’re not the only ones who’ve been debating, just search of the web on this subject, and you’ll find no shortage of opinions.
This is great food for thought about security, and while the consumer’s privacy is paramount in the business of mental health and substance abuse treatment, it seems to me that the professional’s privacy deserves some respect. And I think that’s the point, professionals spend a considerable amount of time and energy learning their craft, and the subtleties of what they do may be lost on a casual reader, followed by misconceptions that could affect the professional’s business or reputation.
I found these revelations fascinating comments on how our world is changing and Facebook is taking over the world. It will be interesting to watch this issue escalate.
Read more →A post on Linked In shared a consultant’s opinion that enterprise software breeds evil.
Well, now, that’s just nonsense. Enterprise software is designed for an agency, in my interest an Electronic Health Record (EHR) for mental health or substance abuse treatment organization, and the software helps people get their jobs done, meet regulatory requirements, assure billing gets done so everybody gets paid, and another very important thing. It may be tempting to rely on memory of a case record rather than go to the chart room to review the consumer’s chart prior to a session. That can be not-so-good; the EHR eliminates trips to the chart room to see previous assessments, progress notes and treatment plans, conceivably bringing a more educated professional into a session and improving the consumer’s likelihood of getting better.
Where does this perception of enterprise software’s evils originate? If I rely purely on anecdotal information, it comes from the customer’s experience with poor implementations. I’ve implemented, been cursorily involved with, and heard of a few EHR implementations, where not every person on the team followed all the advice that ultimately has the professional/consumer relationship in mind. And that shortcoming includes both vendor and agency. Poor planning is the usual culprit.
Over the weekend I went to scenic Boston, MA and attended the NIATx/SAAS conference and was able to sit in on a couple consultants’ sessions about implementing EHRs. I also talked with several vendors, and made an interesting discovery. The “middle tier” of software vendors has come of age. These are software companies that aren’t so big that they’re priced out of a medium-sized agency’s market, or so small they can’t support what they sell. I was particularly interested in the address by keynote speaker David Spong. Another speaker that held my attention was an old friend to substance abuse, H Westley Clark, the director of the Center for Substance Abuse Treatment (CSAT). The consultant’s sessions were interesting insomuch as the questions coming from the audience were the same questions professionals were asking fifteen years ago and before. • How do we pick a software company when there are over 100 vendors out there manufacturing EHRs? • Once we pick an enterprise system, how do we install the doggone software in less than a year and a half? • How do we get professionals to use the system (some are pretty resistant)?
The vendors I talked with in the display area were cordial, very nice guys. I wanted some information that’s key to my business, as it had been a year since I’d updated my records on these vendors. I asked some simple questions, including: • How long have you survived in this tough business? • How many customers do you have, in how many states? • Is your software certified to meet Meaningful Use requirements?
There were more questions, and I plan to address these industry concerns in upcoming posts. Who knows, I may even include some actual information on how to avoid implementation pitfalls and make the experience transparent to consumers…techie consumers are likely to be the only ones interested in this, but for professionals, I think it’s a good subject. I’m thinking about a few reviews of vendors, and sharing my process for narrowing the field of vendors to a manageable few that can be included in a software search.
All in all, the NIATx/SAAS event is a good experience, filled with people who actually care enough about the consumers to stay in business and serve them. I’ll likely attend next time.
…and I software and vendors aren’t evil.
Read more →